Email us
info@letthechildrenhear.com
Call Now
+44 7802 813820
Email us
info@letthechildrenhear.com
Call Now
+44 7802 813820



Josephine, our Paediatric Audiologist, joined LTCH in 2014 as a volunteer and has grown with the team. She is a soft spoken, determined, unstoppable go-getter who loves cooking, business and going to church. Josephine is an audiologist with a background in nursing and has acquired skills in management and leadership. She is very dedicated to her work and it is clearly evident that she loves working with children. She develops a good rapport with her hearing aid clients and strives to provide the best care possible for every child that she sees in the clinic. To the rest of the team she is affectionately called Jojo.
Ruth our administrator spoke to Jojo and this is what she had to say.
What inspired you to do Audiology?
I was invited to attend a 6 month basic audiology training course organised by a team from the Netherlands called Kentalis Academy. I was among the few students that had this opportunity and this experience totally changed my life. I picked interest in this particular field and decided this was something I would love to do. My cousin Josephine Likichori has also been a very big inspiration to me.
How has your journey in Audiology been so far?
It has been like a dream because the cost of the course was very high and I wasn’t sure where I was going to get all the money from but somehow the money came through. We were only 3 students in our class. The course meant balancing work with the academic school work. It included a lot of reading and hard work. Overall it has been an exciting and fulfilling journey studying something you are passionate about.
How has your work with LTCH contributed to your Audiology journey?
LTCH was a amazing opportunity that came my way. It has been a platform for me to learn more and have hands on paediatric experience during my training which many don’t have the opportunity to get because of the nature of this field. The opportunity for me to work with and learn from senior audiologists from the UK has really gone a long way to giving me a lot of good exposure to paediatric audiology. The bigger plus was the opportunity to be employed immediately after school. I am forever grateful to LTCH.
Future dreams. Where do you see yourself in the next few years?
I see myself developing in audiology with a special interest and expertise in paediatrics. I would love to grow and also get involved in consultation work and doing tutorials. This is my future aspiration.
Josephine graduated with a Diploma in Audiology as the best performing student not only in her class but in the whole institution. LTCH is proud to have Josephine as part of the team. Her dedication to her work and to the children is inspirational.



Daniel Ssebagala our nurse highlights a case from the ear clinic where we treat and manage children with common ear diseases.
I get to deal with various kinds of cases but I had never seen something this severe. It was already 5pm, we had cleaned up and were preparing to head home when this little 2 year old boy was brought to the health centre. Because we particularly deal with children, we are often mistaken to be the Paediatric Department. We thought of sending him to the outpatients department but we knew he wasn’t going to get any help based on the time he had arrived. His whole body was covered with wounds which were becoming septic with a bad smell. The worst was in the ears. He was diagnosed with an outer ear infection (Otitis externa) and generalised bacterial infection. The little boy kept scratching his body.
The mother brought him wrapped in a bed sheet because he couldn’t wear clothes as they would stick to the wounds and get mixed with the blood. When asked whether they had got any treatment, the mother told me they had been going to a nearby clinic. The child had been getting injections for over a week with no improvement but they had no idea what medicine they had been administering. They had spent a lot of money. We managed it in our clinic with open dressings and cleaned all the wounds with antiseptic solution. We gave him oral antibiotics, and some antibacterial, antifungal and steroidal cream to apply to the wounds.
By the 2nd visit, the child was much better, and his wounds were drying up. He actually came wearing clothes. I was excited to see how the child was progressing well. You could see the smile on the mothers face. Experiences like this make me enjoy my work at the ear disease clinic. People from different places are being referred to ear clinic because of the kind of quality service being offered. With more health workers being trained to manage common ear diseases, many more children will be able to access these kinds of services. Thank you to everyone who supports us in our work.

This story demonstrates to those that give and support our organisation that we are making a difference to the lives of children like Tonny.
Katende Tonny is 8 years old. He was brought to the clinic by his mother who had concerns about his hearing. She hadn’t been living with her son for a certain period of time because of the nature of the work she was doing. Tonny was born with normal hearing but the period when he wasn’t living with his mother couldn’t be accounted for. Tonny would respond to his name but could barely say a word. The necessary assessment and diagnostic tests were carried out by our audiologist which indicated that he had bilateral severe to profound hearing loss.
Due to our limited supply of reconditioned digital hearing aids we have to assess the suitability of each child and the benefit if any,that they are likely to gain. However with the recent donation of brand new analogue hearing aids we decided to trial them on Tonny. Surprisingly, Tonny had made so much progress when he returned for his review appointment. His mother reported that while wearing the hearing aids he would say simple words like girl, yes mummy (wanji mama),come here (jangu),give me (mpa).
He could also count from 1 to 5. He is no longer the shy boy we met the first time he came to the clinic, he is much happier,confident and very excited. We believe with the support of our speech and language therapist, Tonny’s confidence and communication skills will improve further. He is currently awaiting assessment.
Tonny’s parents were encouraged and told to prepare to get him back to school but that he would need a lot of ongoing support to pick up where he left off. His mother is spending a lot of time with him at home to teach him basic words. Tonny’s hearing levels will be closely monitored as he continues his rehabilitation. In the future he may be considered a suitable candidate for digital hearing aids.
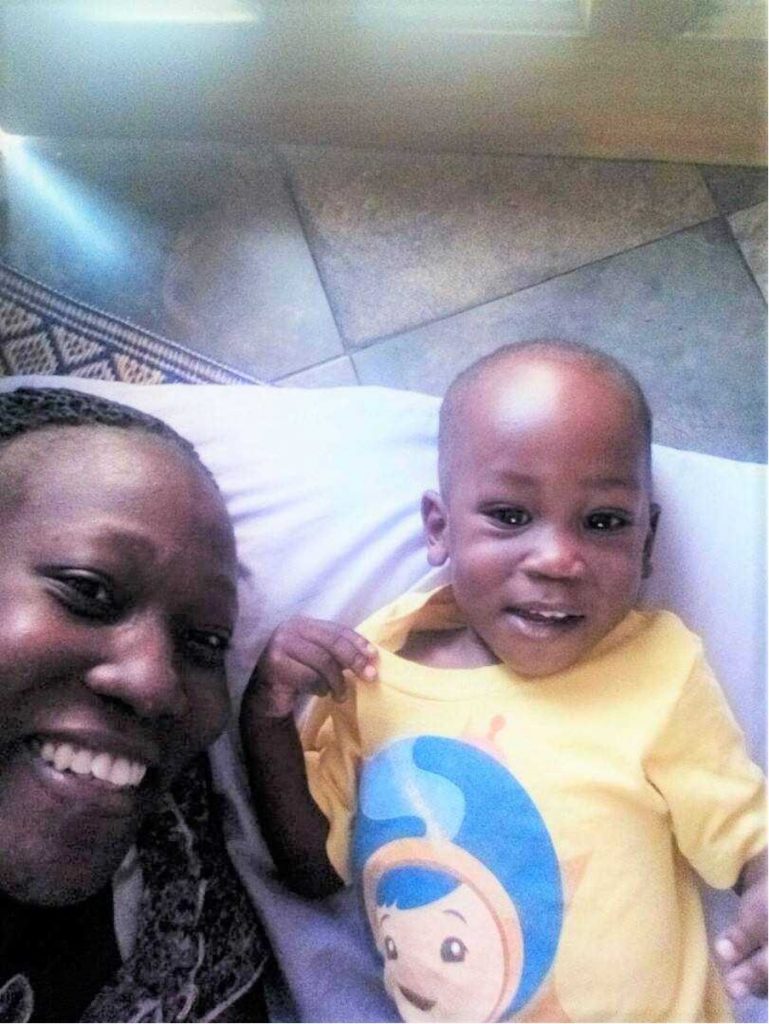
Ruth is our administrator in Uganda and has a son called Jethro Christian who is 16 months old. She would like to share her recent personal experience about how the knowledge she has gained while working with IHCC has opened her eyes as a mother of a young child.
‘During the month of January, my son fell sick, he tested positive for malaria and had an infection. While at the hospital, the doctor instructed the nurse to put my son on an intravenous drip but I had no idea what medicine was going to be administered through the drip.
I kept prompting the nurse to let me know what medicine she was administering but in vain. After a long struggle, we got to know he had been put on Quinine. My experience of seeing the severe effects of this drug, such as sudden onset of irreversible hearing loss in some of the children that have come to the clinic, had made an impression on me and I knew there were other options available.
We requested that another drug be used and we made sure he took a lot of fluids. Currently the government in Uganda is no longer recommending quinine as a frontline drug for management of malaria apart from severe and complicated malaria and where there is no other drug of choice. It also has to be administered in the correct dosage.
Gentamicin was also given to my son to manage the infection but with the experience at the clinic I knew it also had to be administered with precaution. My son has recovered but I intend to bring him to the clinic for a hearing test just to check his hearing is ok. I am sure the story would have been very different if I still lacked the knowledge I have now gained. Unfortunately, some of these things are still happening in our communities therefore there is a continued need for more education and vigilance throughout all sectors of our community’.
Sitting patiently while an impression is being taken to make an ear mould for his new hearing aid
One of our children delighted with her new hearing aidWe held our (delayed) “World Hearing Day” celebration (the actual day is 3rd March each year, but none of us were in Uganda yet!). Which has also brought quite a number of new children in to our clinic. We are thankful for the media coverage; IHCC was featured on television news, in newspapers as well as on the radio. We have already seen a few new children whose parents heard about IHCC from the radio, who have been able to receive the necessary treatment from our clinic. We look forward to 2 more outreaches planned for the next 3 weeks





For today’s blog I want to share the story of one of my patients. Sarafina and her mother came along to out “World Hearing Day” outreach. Sarafina is now 13 years old and had lost her hearing 6 years ago while fleeing the war in the Congo. They travelled for 2 weeks through forests, at times they had to run from gun fire and explosions at a close range. Lack of knowledge about hearing loss as well as lack of available services meant that she has not seen anyone about her hearing. Her hearing test revealed a bilateral sensorineural hearing loss- this means that there is permanent damage to the hearing pathways. Fortunately hearing aids would offer her some improvement.
The news was tough on her mother emotionally as she had presumed that we would be offering medical treatment to immediately restore the hearing that has been lost. After some counselling (involving three different language translations), Sarafina and her mother decided that they would like to try the hearing aids, impressions were taken and sent off for moulds to be made. A week later we were able to fit her with two new hearing aids.
So far we are pleased with how she is responding with her hearing aids. Safari’s progress will be followed up over the next few weeks as she adjusts to her hearing aids. We hope that her hearing aids will help her to connect with the people around her, and make it easier for her to hear in school, setting her up for a brighter future!
April 2016
A quick introduction: I’m Katie, a South African audiologist. I have been locuming in Ireland and the U.K. for the past year and a half, which has given me the flexibility to come out to Uganda for these 5 weeks to volunteer. A few years ago I saw the right tweet at the right time which got me in contact with IHCC, and here I am! I look forward to sharing my experiences with you through this blog!

It has already been 2 incredible weeks in Uganda with IHCC. We have been making our way through the waiting list of children that have accumulated over the last few months- ABR’s, hearing tests, hearing aid follow ups, new ear mounds and we recently started with the hearing aid fittings. We have some very happy kids with their “new ears”! The audiology clinic has really come along, we are now able to take our own ear mould impressions (instead of sending the children off to the private clinic), which has reduced the time between hearing assessments and hearing aid fittings. We now also have our own laptop and software to program the hearing aids, which means that the hearing aids can be programmed according to each child’s individual hearing test, and adjustments can be made in the session.
Gentamicin was also given to my son to manage the infection but with the experience at the clinic I knew it also had to be administered with precaution. My son has recovered but I intend to bring him to the clinic for a hearing test just to check his hearing is ok. I am sure the story would have been very different if I still lacked the knowledge I have now gained. Unfortunately, some of these things are still happening in our communities therefore there is a continued need for more education and vigilance throughout all sectors of our community’.
April 2016
Activity in our clinic was winding down with only a few more days before we would close for the Christmas break. It was a quiet afternoon at the Health Centre and not so many children were coming to the clinic. We heard a very excited group of people outside our clinic who had decided to take a few pictures in front of the door We were wondering what the excitement was really about and went to see. Then we understood why, it wasn’t just one baby but 3 beautiful newborn baby girls. Yes triplets had just been discharged from the maternity unit and were just having their photos taken before going home. After their ‘Kodak’ moment, the family were invited in to the clinic to have their babies’ hearing screened before going home. They consented to the test and asked many questions.

It was a great opportunity to provide health education to the mum around the issue of childhood hearing loss The babies were born at full term and there were no identified risk factors for hearing loss. The babies were screened, one of them passed the test while the other two didn’t We asked the mum to bring them back, which she did, and the other two babies passed their second screening test. The mum was very happy to hear this good news. However this is just the beginning and we encourage all mothers to continue to monitor their child’s hearing throughout childhood’.
One of the most important aspects of newborn screening is that it provides a platform on which to educate new mothers about their child’s hearing and language development. Our aim is to ensure that every mother leaves our clinic with information about their child’s hearing and the services we offer. This information is clearly being spread throughout Uganda, among friends and relatives. We are beginning to see a change in health seeking behaviour; parents are beginning to access earlier intervention for suspected hearing loss.This is great news!
Wed, Feb 10, 2016
We may well be able to coincide the launch with our planned community outreach to commemorate this year’s WHO World Hearing Day in March, the theme of which this year, is CHILDREN!

Gentamicin was also given to my son to manage the infection but with the experience at the clinic I knew it also had to be administered with precaution. My son has recovered but I intend to bring him to the clinic for a hearing test just to check his hearing is ok. I am sure the story would have been very different if I still lacked the knowledge I have now gained. Unfortunately, some of these things
Our medical team in Kampala have spent the last three months working to secure the purchase of a good second-hand ambulance that meets both the charity’s requirements and is within the budget allocated to us in the rotary grant.
On recommendation it was decided to go with the purchase of an ambulance from Japan.
Finally, in December, we found one that suited our specifications. An order has been placed and the vehicle is on it’s way from Japan and due to arrive in Kampala towards the end of February.
It is hoped that we will be ready to launch the services of the mobile clinic sometime in March.
We may well be able to coincide the launch with our planned community outreach to commemorate this year’s WHO World Hearing Day in March, the theme of which this year, is CHILDREN!
are still happening in our communities therefore there is a continued need for more education and vigilance throughout all sectors of our community’.
Ruth is our administrator in Uganda and has a son called Jethro Christian who is 16 months old. She would like to share her recent personal experience about how the knowledge she has gained while working with IHCC has opened her eyes as a mother of a young child.
‘During the month of January, my son fell sick, he tested positive for malaria and had an infection. While at the hospital, the doctor instructed the nurse to put my son on an intravenous drip but I had no idea what medicine was going to be administered through the drip.
I kept prompting the nurse to let me know what medicine she was administering but in vain. After a long struggle, we got to know he had been put on Quinine. My experience of seeing the severe effects of this drug, such as sudden onset of irreversible hearing loss in some of the children that have come to the clinic, had made an impression on me and I knew there were other options available.
We requested that another drug be used and we made sure he took a lot of fluids. Currently the government in Uganda is no longer recommending quinine as a frontline drug for management of malaria apart from severe and complicated malaria and where there is no other drug of choice. It also has to be administered in the correct dosage.
Gentamicin was also given to my son to manage the infection but with the experience at the clinic I knew it also had to be administered with precaution. My son has recovered but I intend to bring him to the clinic for a hearing test just to check his hearing is ok. I am sure the story would have been very different if I still lacked the knowledge I have now gained. Unfortunately, some of these things are still happening in our communities therefore there is a continued need for more education and vigilance throughout all sectors of our community’.

© 2020 Let the Children hear Design and Developed by Themes Glance